I’ve tested for MTHFR, I don’t have it, now what?
You still need to optimise your folate!
If you’ve been tested for the MTHFR gene(s) in the hopes that it may have provided you answers to your difficulties with conceiving, only to discover you don’t actually have problematic MTHFR SNPs that can commonly underly unexplained infertility – this is great news! However, this doesn’t mean that the folate that you’re consuming as part of your prenatal preconception planning is actually right for you or its being absorbed into the cell. Because the MTHFR gene is not the only pathway influencing how your body responds to or deals with folate and folic acid.
You see, not all folate is created equal.
For decades now, health professionals have been routinely recommending folic acid as part of a woman’s prenatal regime, as it is well known that optimal folate will help to prevent neural tube defects. What this advice fails to take into consideration is whether or not you can make or convert your folate into the form the body recognises and uses for essential functions. So too, an overload of folic acid may slow your pathway down.
The other important factor to consider is your Vitamin B12. If you don’t have enough B12, you won’t use your folate. So many people have genetic polymorphisms that affect their metabolism and transport of Vitamin B12. You may be one of them, so you can take the right form of folate and the right amount, but you’re not using it.
If this information is new to you, we recommend you watch our free webinar that explains the difference between folic acid and folate:
Folate vs Folic Acid Webinar
Folate: An Umbrella Term
Folic acid is technically not ‘folate’, it’s more like a synthetic ‘doppelganger’ – ie. looks similar, functions similarly, but certainly not a 100% identical replica. And, as science has progressed in understanding this molecule, it seems medical advice has been lagging behind.
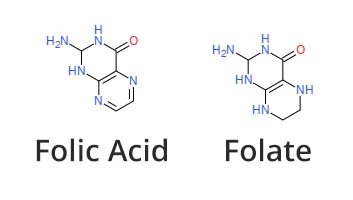
The two extra lines you see in the bottom hexagonal structure in folic acid is what make it a ‘stabilised’ molecule, capable of being mass produced. This is why folic acid has been the most commonly utilised form of ‘folate’ in supplementation. Because it’s a synthetic version and has been completely oxidised, it means it’s more stable to be placed into a supplement with a shelf life that’s predictable and thus ‘safe’.
The terms folate and folic acid have been used interchangeably for many years, even in scientific publications, but as you can see, there are some important differences between the two, and it can be vitally important to understand which is being referred to.
Folate: An Umbrella Term
The problem for many couples is; unmetabolised folic acid.
Unmetabolised folic acid is the folic acid that’s building up in the system because it’s not being used. Research says this may actually cause a pseudo MTHFR deficiency and so down regulate the enzyme that’s meant to be making your active folate.
There’s simply not enough emphasis being placed on unmetabolised folic acid and the potential this has to disrupt successful fertility. In fact, to this day health professionals may see off-the-charts folate in a blood test and simply assume that person is eating a bulk amount of leafy greens to return that result. But when you dive deeper, you can see, this is often not the case at all. It’s folic acid, or folate that is not moving through its metabolic pathways the way it should.
You see, it’s true that the body will recognise folic acid as ‘similar enough’ and will convert it slowly through the pathways of enzymes (eg. MTHFR – Methylenetetrahydrofolate reductase) – which is why checking if you have a genetic variation that impairs this pathway is important. But the story doesn’t end there.
Synthetic folic acid is largely metabolised by the liver by an enzyme called dihydrofolate reductase (DHFR), so;
- First of all, liver health is something everyone should pay attention to, but especially women wishing to have a baby, because the liver has a huge burden of work to do when it comes to managing the hormonal surges that facilitate pregnancy.
- Secondly, it is possible to also have SNPs (single nucleotide polymorphisms) that influence DHFR, just like we have the MTHFR SNPs that can impact folate.
- And, further to that, folic acid has been demonstrated to have the potential to inhibit the DHFR pathway (which ironically is the necessary step required to convert it to the bioactive folate for the purpose of fertility benefits).
COMPREHENSIVE FERTILITY ASSESSMENT TOOLKIT
This can all lead to excess, unmetabolised folic acid. Too much coming in from dietary fortification and supplements combined with a lack of, or an impaired system of pathways to metabolise it into the form of folate needed for essential bodily functions, in particular, the pathways that depend upon it for fertility.
What this means is, folic acid may not be effectively converted and is therefore left in circulation where it can impact immunity, certain medications and decrease the body’s capacity to convert dietary folate leading to a ‘pseudo MTHFR – like state’.
When this happens, we need to give the body the opportunity to clear this build up of unmetabolised folic acid by removing all sources and taking that burden from the body, whilst also supplementing with forms of folate that the body can use quickly and efficiently.
So, how can we maximise fertility?
One of the best things we can do is bypass all of these potential issues by supplementing with prenatal vitamins that only contain activated folate.
The most biologically active form of folate is 5-MTHF (also known as methylfolate). You see, supplementing with folic acid, or getting it from fortified food products like bread and breakfast cereals – the body is passing it through enzymatic metabolic pathways (MTHFR, DHFR) with the intention of converting it to 5-MTHF so it can be absorbed and utilised by the body. So if you have a problem, it’s more use to the body to actually take the form of folate that the body will use.
It’s highly recommended for couples experiencing infertility to remove all sources of folic acid from their supplement regime, and from their diet (in fortified foods, such as commercial breads and flours) and look to replace it with 5-MTHF or folinic acid. This helps to maximise the amount of biologically active folate available to the body for the purpose of making the quality DNA needed when making a baby.
We specifically created preconception starter products which consists of our Prenatal Methyl, Methyl B12 Drops and our Liquid Methyl Folate Drops to help couples optimise their folate status for natural and assisted fertility needs.
And remember, this doesn’t just apply to females. All babies gain 50% of their DNA from their father, so it’s vitally important for males to be on top of their folate status too. Prenatal Methyl is a unisex formula, suitable for both men and women.
Remember, you are not alone.
MTHFR Support has helped thousands of women around the world to unravel the underlying biochemical or genetic factors that may be contributing to infertility. Join our community to share in the collective wisdom of couples who, like you, have been searching for answers and support to achieve a healthy pregnancy.
If you would like to join our ‘Your Baby course’ community why not sign up for our course today to get the support and assistance you need to evaluate/plan and prepare for your pregnancy. Our fertility team will be standing by to support you along the way.